|
Nonoperative Treatment
Once an ulnar collateral ligament tear is diagnosed, the player is given options regarding how to heal the ligament. There are surgical and non-surgical methods, and the player's path to health is generally influenced by his or her individual situation. Factors such as prior injuries, time of the baseball season, and player potential are taken into consideration.
Nonoperative treatment of the UCL is often recommended at first to avoid the long road associated with surgery. Specific protocols for this treatment can vary, although they all are likely to contain a period of rest followed by rehabilitation. A program suggested by Rettig et al. (2001) can be seen in Table 1. Medication, ice, and a splint accompany the rest phase. Once pain is absent, the player then progresses into a throwing program to strengthen the arm.
|
Table 1: Nonoperative Treatment for Ulnar Collateral Ligament Injuries of the Elbow |
|
Phase |
Treatment |
|
I |
Rest from throwing for 2 to 3 months. |
|
|
Antiinflammatory medication. |
|
|
Ice elbow for 10 minutes 4 times daily. |
|
|
Long-arm splint or improved range of motion brace at 90 degrees at night, wear as needed to control pain during the day. |
|
|
Active and passive range of motion exercistes for flexors and pronators. |
|
|
|
|
II |
If pain free: |
|
|
Discontinue splint or brace. |
|
|
Progress upper extremity strengthening program to all muscle groups. |
|
|
Begin throwing progression at 3 months. |
|
|
Elbow hyperextension brace may be used for throwing and lifting. |
A recent study conducted on thirty-one athletes with ulnar collateral ligament injuries sought to determine the effectiveness of the nonoperative treatment option. The investigators also examined specific factors that may predict the athlete's ability to return to play without surgery. The average age of participants in this study was 18 years and the average follow-up was 29.8 months. Forty-two percent of the athletes (13 of 31) were able to return to their sport at an average of 24.5 weeks after diagnosis (Rettig et al.2001). Although this rate of return is lower than that consistently seen with surgical reconstruction, it is high enough to elicit considerations by doctors to recommend this type of treatment in some cases before turning to surgical methods. The researchers collected data regarding the duration of symptoms at the time of examination, age of athlete at onset, and whether onset of symptoms was acute (instantaneous) or insidious (over time). All three aspects did not have significant differences between those who effectively returned after nonoperative treatment and those who did not (Rettig et al. 2001). Their interpretation suggests that the characteristics examined would not aid the doctor in predicting whether the nonoperative treatment will be successful.
Surgery Decision
The more severe option provided to athletes with a torn ulnar collateral ligament is surgery. This can occur once nonoperative treatment has failed or if the doctor decides that immediate surgery is the best choice based on the patients history or situation (time of the baseball season). This is a large commitment on the athletes behalf since it will require extensive rehabilitation, and thus the doctor will need to discuss all aspects of the surgery with the patient, including if they have a future in baseball. In 1981, while the technique was still in its infancy, Dr. Jobe determined that Tom Candiotti was in need of the surgery to fix his ligament. Jobe recalls, He was a young guy in [Class A], and I remember asking him Do you think youre a real prospect?. Thanks to the opportunity Jobe afforded him, Candiotti became a successful major league pitcher with over 150 wins. Some college athletes, however, are forced to face the reality of their abilities. If they do not have a possible career in baseball and have used up some of their eligibility, many collegians will elect not to have the surgery.
There is evidence that avoiding surgery will not have a negative affect on the persons lifestyle. Elbow dislocation often results in a ruptured ulnar collateral ligament, and nonoperative treatment of this injury yields positive results (Josefsson et al. 1987). Nonetheless, if this person intends to participate in recreational sports, it is recommended that they use a stabilizing brace. This will protect the ulnar nerve from injury due to the elbow instability (Conway et al. 1992).
Surgical Technique
Although variations exist in the surgical procedure for reconstructing the ulnar collateral ligament, Conway, Jobe, Glousman, and Pink (1992) explained the basic method in the article Medial Instability of the Elbow in Throwing Athletes. A few additional steps are articulated in more recent articles.
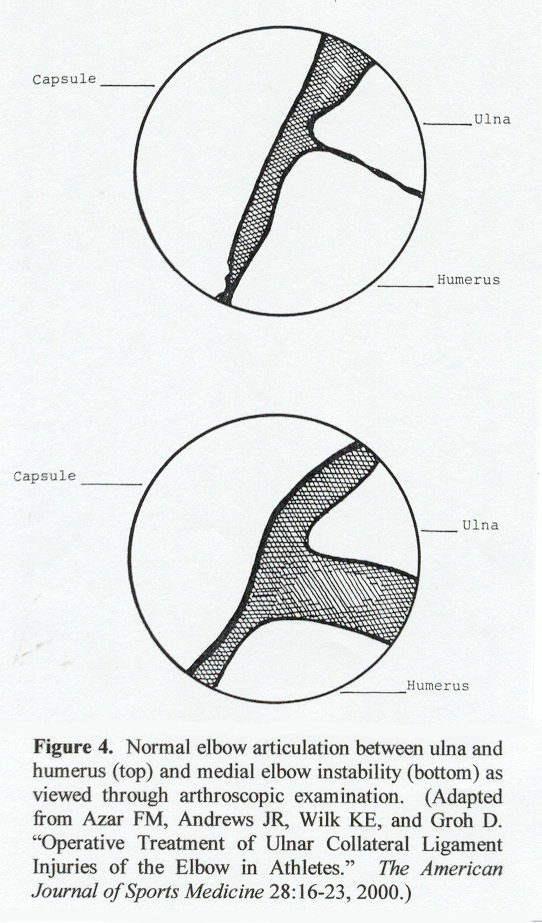
First the athlete is anesthetized, and both elbows are tested for range of motion, carrying angle, and instability. A padded pneumatic tourniquet is then applied to the upper arm, followed by sterile preparation and draping. Doctors recently have decided to procede with a brief arthroscopic examination to confirm the elbow instability. The anterior twenty percent of the anterior band is viewed while valgus stress is applied at seventy degrees of flexion. Evidence of a tear is seen as two millimeters or more of laxity, seen in Figure 4 (Azar et al. 2000). Following the arthroscopic exam, the arm is then repositioned and prepared for surgery.
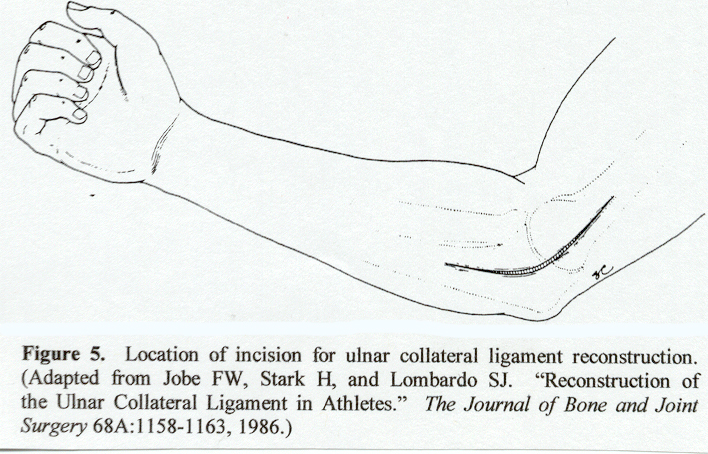
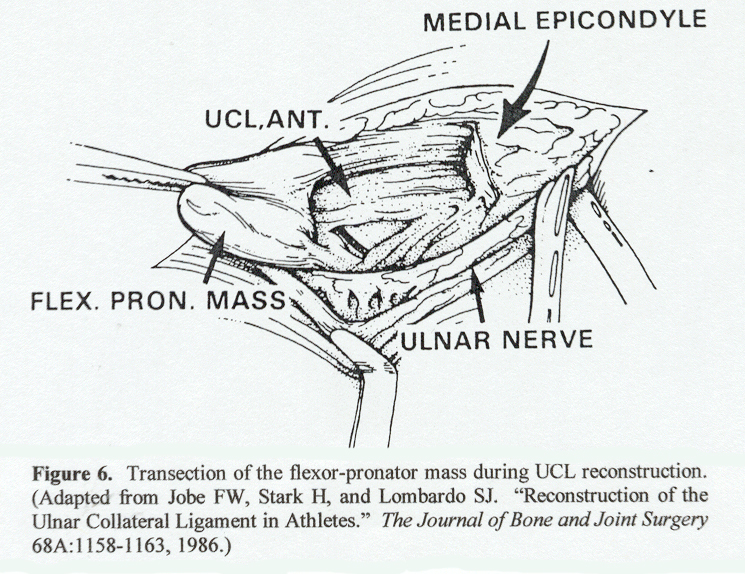
Centered over the medial epicondyle, a ten-centimeter incision is used to expose the elbow joint, with care taken to protect the sensory nerves in the area (Figure 5). The mass of the flexor-pronator muscle is then incised one centimeter distal to the medial epicondyle. This transection of the origin of the flexor-pronator bundle and distal reflection provides a greater exposure of the ligament (Figure 6). An alternative exposure method will be discussed later.
Now that the UCL can be seen, any calcification within ligament is removed. The doctor next identifies the ligament tear. If no tear can be seen on the external aspect of the ligament, an incision is made into the ligament in line with the fibers to search for an undersurface tear (Azar et al. 2000). The medial antebrachial cutaneous nerve is protected with a Penrose drain, and the ulnar nerve identified. Care is taken to release the ulnar nerve through a dissection of the arcade of Struthers, and protect it with a Penrose drain. The nerve can then be manipulated during surgery. At this time, any remaining loose bodies or osteophytes in the elbow joint are removed.
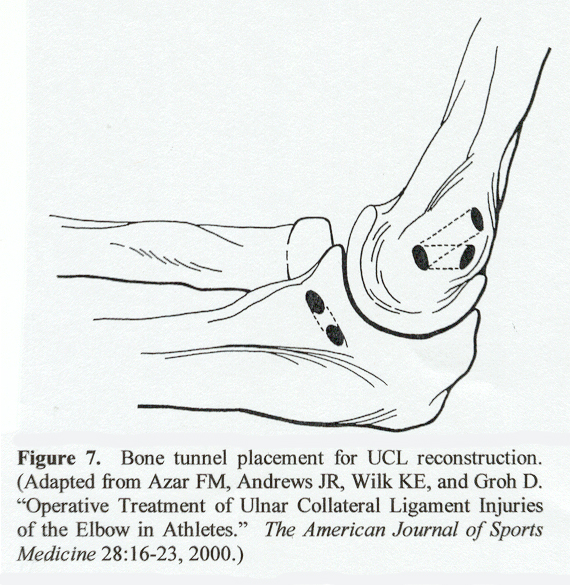
Next, 3.2-millimeter holes are drilled in the medial epicondyle and the ulna using a slow-speed drill with a drill guide (Figure 7). These tunnels, placed so that the graft would not rub on the medial epicondyle or the bony prominence of the ulna, correspond to the attachment sites of the torn ulnar collateral ligament.
The ensuing step in this procedure is the harvesting of the tendon graft. Seventy five percent of the population have a palmaris longus, a tendon that originates at the medial epicondyle of the humerus and inserts on the transverse carpal ligament and palmer aponeurosis (Wheeless Textbook of Orthopaedics 2001). It is responsible for weak hand flexion at the wrist. Prior to surgery, the doctor determines if the tendon is present by active opposition of the thumb against the little finger. Palpation should allow the physician to assess if the tendon will be big enough, and it is generally taken from the ipsilateral side. The technique of procuring the palmaris longus tendon is described in Wheeless Textbook of Orthopaedics. First, a transverse wrist incision is made and the surrounding tissue is spread away in order to identify the tendon. A second transverse incision is then made about eight centimeters proximal from the first wound. The tendon is then pulled from both cuts to establish that the correct tendon has been isolated. A third incision is generally made to ensure that the graft will be long enough. The tendon is then removed, cleaned with a tendon stripper, and placed in saline. For patients that do not possess a palmaris longus tendon, either the plantaris or a strip of the Achilles tendon may be used. Surgical results were not significantly different between the various types tendon grafts (Conway et al. 1992).
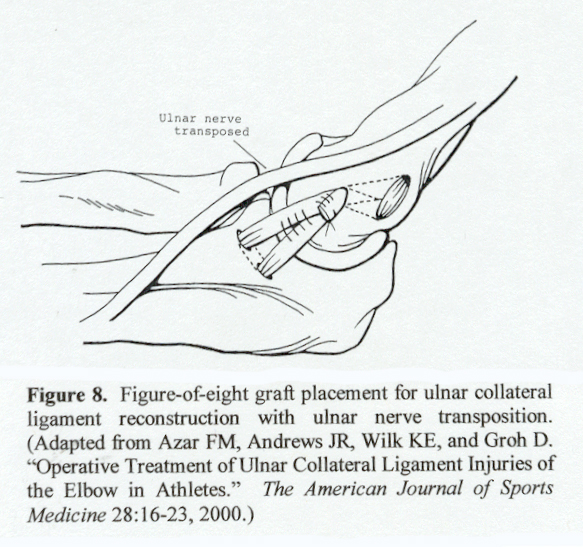
Then the tendon is passed through the bone tunnels in a figure-of-eight manner with a suture passer (Figure 8). This allows it to be a functional substitute for the ulnar collateral ligaments anterior band. If enough length remains, the tendon may be passed through the tunnel again for added support. The graft is then pulled tight and sutured to itself. Additional strength is gained by suturing any remains of the original ligament to the tendon graft.
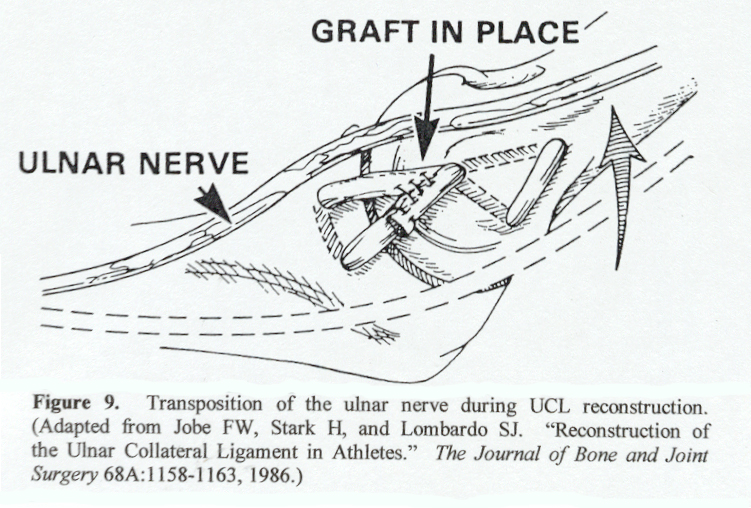
After successfully replacing the ulnar collateral ligament with a tendon graft, the surgeon performs an ulnar nerve transposition by transfering the ulnar nerve anterior to the medial epicondyle as seen in Figure 9. The ulnar nerve placement is examined to confirm that there is no nerve impingement. The flexor-pronator muscle bundle is then reattached over the nerve to help keep it in place (Jobe et al. 1986). The elbow is subsequently tested for full range of motion and a gentle valgus stress is applied to test the reconstructed ligament. If the surgeon is satisfied with the results, the tourniquet is released and the wound is closed. The arm is placed in a well-padded posterior splint with the elbow in ninety degrees of flexion (Azar et al. 2000).
|