Anatomy of the Elbow
A basic knowledge of the elbow complex is essential in order to understand the injury of the ulnar collateral ligament. The elbow joint involves the meeting of three bones: the humerus (upper arm) and the radius and ulna (lower arm). The distal humerous is triangular and consists of a central trochlea supported by two columns, the lateral epicondyle and medial epicondyle. These structures serve as attachment sites for muscles and ligaments. The proximal ulna has a trochlear notch that runs from the coronoid process to the olecranon process.
The ulnar collateral ligament (sometimes referred to as the medial collateral ligament) is considered the prime stabilizer of the joint (Reckling 1990). It has a fan-shaped configuration consisting of the anterior and posterior bundles, and the transverse ligament (Figure 1). The anterior bundle connects the lateral side of the medial epicondyle and the medial edge of the coronoid process. The posterior bundle connects the medial epicondyle to the medial edge of the olecronon process, and the transverse band serves a support function.
Mechanism of Injury
A torn ulnar collateral ligament was first examined in javelin throwers. A 1946 study by Wille Waris concluded that the motion of throwing a javelin damaged the inner aspect of the elbow, including the ulnar collateral ligament. Waris noted that 12 of 17 world-class javelin-throwers had exhibited elbow problems, almost all within their first year of competition. This arm movement is similar to that executed by baseball pitchers.
The motion involved in throwing an overhand baseball pitch can be broken down into five phases: wind-up, early cocking, late cocking, acceleration, and follow-through. Fleisig, Andrews, Dillman, and Escamilla (1995) conducted a study at the American Sports Medicine Institute testing elbow and shoulder kinetics. They defined elbow kinetics as "the summation of all internal force and torque applied to the forearm by musculature, osseous, and other tissue." During the late cocking phase, the average maximum varus torque (rotation force exerted toward the midline of the body) of the twenty-six subjects was 64 ± 12 Newton- meters. In the acceleration phase, depicted in Figure 2, the average maximum varus torque was 61 ± 11 Newton-meters (Fleisig et al. 1995). Conway et al. (1992) proposed that the curveball might be responsible for a large amount of the injuries to the medial elbow. Although a curveball generates less torque on the elbow than a fastball, the deceleration phase for a curveball is much shorter. This increases the angular velocity in the elbow after the ball is released.
When measuring the ligamentous contributions to the stability of the elbow joint, Morrey and An (1983) determined that the ulnar collateral ligament (UCL) was responsible for generating fifty-four percent of the total varus torque necessary to resist valgus motion. Fleisig concluded that the UCL produced fifty-four percent of the 64 N-m varus torque, a total of 34.6 N-m. Cadaveric testing showed that the amount of torque the UCL could produce before failing was 32.1 ± 9.6 N-m (Dillman et al. 1991; cited in Fleisig et al. 1995). This maximal torque in cadaver ulnar collateral ligaments is less than the torque calculated by Fleisig which indicates that pitchers are exerting excess stress on their ulnar collateral ligaments during pitching.
Some factors may help to slightly lessen the strain placed on the UCL. In what is called "dynamic stabilization," muscle contraction during the acceleration phase by the triceps and anconeus muscles compress the ulnohumeral joint and add stability while throwing (Fleisig & Barrentine 1995; cited in Ellenbecker & Mattalino 1997). This stability is often compromised by factors such as poor mechanics, lack of flexibility and conditioning, and fatigue from overuse which will put pitchers at a greater risk of injury (Jobe & Kvitne 1991; cited in Ellenbecker & Mattalino 1997).
An ulnar collateral ligament injury can occur in one of two ways. A sudden event may immediately cause the athlete to stop playing. However, the more common mode of injury is a slow deterioration of the ligament (Spivak 1999). Loss of control and increasing pain can eventually lead a pitcher to seek medical help after months or years of discomfort resulting from small tears. The athletes may assume that the soreness is a normal aspect of pitching until they reach their pain threshold and decide to get their elbow examined. Stress on the ligament can cause dissociation of ligament fibers, leading to calcification. The ligament will then become weak and possibly rupture. The ligament is most likely to avulse from the ulnar insertion at the coronoid process, but may also tear midsubstance or from the medical epicondyle (Ellenbecker & Mattalino 1997). The weakening of the UCL combined with the excessive valgus stress associated with throwing places more stress on the ulnar nerve. This can lead to nerve damage accompanying the UCL tear.
Clinical Evaluation
When an athlete seems injured and visits a doctor, there is a general evaluation that proceeds in order to determine the exact cause of his problem. An ulnar collateral ligament injury is not easy to identify. The physician must consider many different diagnostic tests before reaching a decision.
The first step is to take a history of the athlete. The doctor should know all facets of the patient's medical history. This includes prior injuries the ballplayer has experienced, any surgery he has undergone, and the location of the pain. Also, a description of the pain and any associated symptoms such as swelling or numbness, the date of injury, and the origin of the symptoms and pain (single event or progressive onset) are helpful. Specifically when examining the elbow of a pitcher, it is important to know when symptoms occur during the throwing motion and whether the training program or mechanics have been altered (Spivak 1999). This knowledge will allow the doctor to perform an informed and comprehensive physical exam.
Next, the patients active range of motion is examined. The flexion, extension, supination, and pronation should be compared between the injured and healthy elbow. This helps to determine what is normal for the athlete and whether the injury is affecting pain or increasing or decreasing range of motion. The active movement is not conclusive evidence since it includes contractile and noncontractile tissue (Malone 1997).
The passive range of motion is subsequently tested, and the noncontractile tissue can be studied. With the patient relaxed, the doctor then moves the arm in the same motions as when the active movement was assessed in order to observe whether the injured arm is affected. If the movement is excessive, it is possible that there has been damage to surrounding muscle or connective tissue. Conversely, the movement can be limited in two ways. Capsular limitation generally will affect both opposing motions, such as flexion and extension. This is normal when joint swelling is present which could have been caused by various factors. Noncapsular limitations, on the other hand, restrict one aspect of the joint more than another. The most common noncapsular limitations are loose bodies of bone or cartilage in the joint (Malone 1999). This testing is important because throwing pain can also be caused by olecranon osteophytes, flexor-pronator mass injuries, ulnar nerve injuries, and stress fractures of the ulna (Timmerman et al. 1994).
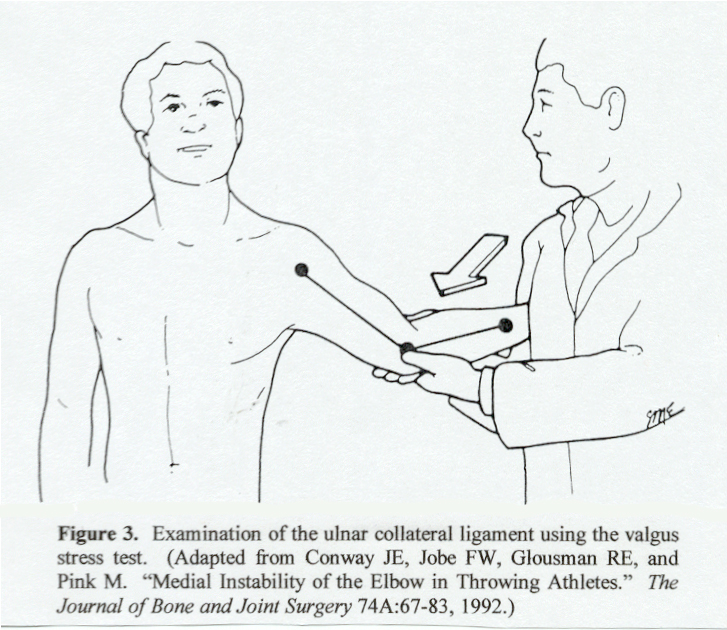
To directly test the integrity of the ulnar collateral ligament, a valgus stress test is always performed (Figure 3). The elbow should be in approximately thirty degrees of flexion in order to unlock the olecranon process from the olecranon fossa, thus applying the greatest stress to the ligament (Ellenbecker and Mattalino 1997). The physician should hold the elbow and prevent humeral external rotation. The wrist should then be moved valgus (away from the midline) and the doctor should palpate the ulnohumeral joint looking for tenderness over the ligament and increased laxity. A problem with this type of testing is that the full force of throwing may be necessary to reproduce the joint instability (Timmerman et al. 1994). However, in general, this testing is very effective.
Following a positive valgus stress test, the doctor generally recommends more advanced measures in order to make an accurate diagnosis and possibly see exactly where the problem is located. One method commonly used is magnetic resonance imaging (MRI). In a study performed by Timmerman, Schwartz, and Andrews (1994), twenty-five patients with medial elbow pain were examined, and fourteen were found to have UCL tears. Magnetic resonance imaging was one hundred percent accurate for diagnosing full-thickness tears (7 of 7), while only fourteen percent (1 of 7) of partial tears could be seen. Another technique, computed tomography arthrography, involves injecting three milliliters of contrast and six milliliters of air into the joint followed by a CT scan. The CT arthrography was used to look at the same fourteen UCL tears, and it was found to be more accurate than the MRI by looking for a T-sign. This represents dye leaking around the detachment of the UCL while remaining in the intact capsule (Timmerman et al. 1994). One hundred percent of the full-thickness tears could be seen (7 of 7), whereas seventy-one percent of the partial tears were apparent (5 of 7). Although the CT arthrography was more precise, MRI scans have the advantage of being noninvasive and not involving radiation exposure. The authors concluded that CT arthrography was the best method available to diagnose ulnar collateral ligament tears, although the prospect of contrast MRIs may alter that finding (Timmerman et al. 1994).
Rijke et al. (1994) examined 42 injured elbows via stress radiography. The symptomatic and normal elbows were compared regarding the amount of opening in the medial joint when a valgus force is applied. The investigators determined that if the difference between the elbows was greater than 0.5 millimeters, the ulnar collateral ligament was torn. A recent study by Singh et al. (2001) has disagreed with that finding. While probing tendencies for valgus laxity in healthy athletes, the experimenters compared stress radiographs for the dominant and non-dominant elbows. They found that 25 percent of the healthy athletes had a difference in valgus laxity greater than 0.5 millimeters, and concluded that using this value as a cutoff for determining ulnar collateral ligament tears was not effective (Singh et al. 2001).