|
Although Tommy Johns surgery in 1974 was considered successful due to his triumphant return to the major league level, there are multiple aspects of the surgery that have since been challenged. For example, Hyman et al. (2001) suggest that the palmaris longus tendon can be harvested with a single incision at the distal palmar crease instead of the two incisions commonly made. They state this improves surgery because it is faster and there has been no associated morbidity from bleeding or median nerve trauma with this technique (Hyman et al. 2001).
Another minor change is the size and placement of the bone tunnels. Thompson et al. (2001) support a technique that uses a 4.5 millimeter drill bit at the humeral origin of the ligament and a 3.5 millimeter drill bit at the UCL attachment sites on the ulna and humerus. Another change is that the tunnels used to be directed through the posterior cortex but this new method directs the tunnels anteriorly (Thompson et al. 2001). These, however, are small revisions compared to other aspects of ulnar collateral ligament replacement being disputed.
Muscle-Splitting Technique
Jobes conventional method of transecting the flexor-pronator muscle and reflecting it distally has been an effective way to obtain exposure. However, Smith et al. (1996) examined a muscle-splitting approach, suggesting that it is less traumatic to the muscle and could decrease operative time and lessen morbidity immediately after surgery. The goal of the study was to determine a safe zone for the muscle split that would not denervate the musculature.
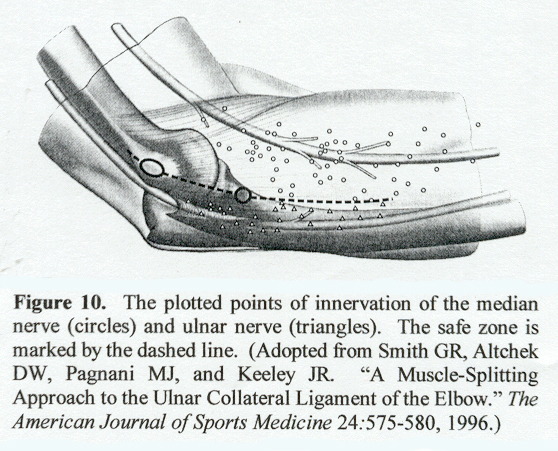
The proposed muscle split is within a raphe between the ulnar-innervated flexor carpi ulnaris and median-innervated common flexor mass (Smith et al. 1996). To find the safe zone, the investigators reflected the flexor-pronator mass of a cadaver toward the ulna to expose the nerve branches entering the muscle. Spinal needles were used to mark the sites of innervation and the muscle was then replaced. The needle positions were mapped in relation to the medial humeral epicondyle, the sublime tubercle of the ulna, and the site of the muscle split itself (Smith et al. 1996). The area safe for performing a muscle-split narrows distally. It begins at the medial epicondyle and runs approximately one centimeter distal to the sublime tubercle of the ulna as seen in Figure 10. Smith and his colleagues tested their findings on 22 patients, and with a minimum follow-up of one year, no patient had evidence of neuropathy. This approach is done without a transposition of the ulnar nerve, although the nerve must be identified prior to splitting the muscle.
In a survey I conducted of orthopedic surgeons involved with professional sports, 9 of 12 (75%) obtained exposure of the ulnar collateral ligament with a muscle-split (Figure 11). Two others (16.7%) preferred to retract the flexor-pronator muscle, and one surgeon cuts anterior to the flexor carpi ulnaris muscle.
Ulnar Nerve Transposition
The initial surgery involved a transposition of the ulnar nerve. In 2000, Azar et al. published the results of 91 ulnar collateral ligament reconstructions. All patients in this study had the UCL transposed subcutaneously and stabilized with a facial sling. Only one of the 91 patients developed postoperative ulnar nerve changes, and this was resolved at 10 months. The authors acknowledge that the ulnar nerve transposition is not necessary, but they feel the procedure has advantages. Along with good results with subcutaneous transposition (79% returned to previous level of play or higher) a transposition is also believed to reduce postoperative ulnar nerve problems and assist with the UCL exposure. Also, some players with torn ulnar collateral ligaments experience ulnar nerve symptoms as part of the injury. Of ten patients entering UCL replacement surgery with ulnar nerve problems, nine experienced resolution of their symptoms after an operation with a transposition.
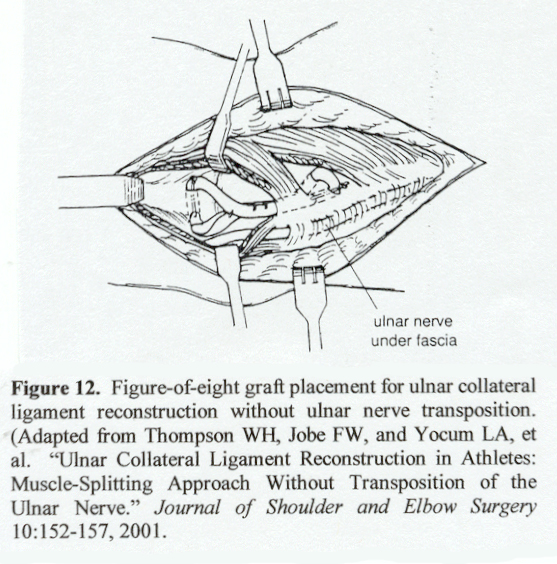
Some results have not been as encouraging. Tommy John needed a second surgery three months after the original one to reposition his ulnar nerve. Conway et al. (1992) saw 15 of 71 (21.1%) UCL reconstruction patients experience ulnar nerve neuropathies after Dr. Jobe transposed the nerve submuscularly. Nine of the fifteen required an additional procedure to address the neuropathy. Dr. Jobe then revised his procedure so a transposition would not be necessary (Conway and Lowe 2001). By not transposing the nerve and directing the humeral tunnels through the anterior cortex instead of the posterior as seen in Figure 12, Dr. Jobe found a way to lessen the risk of nerve injury after surgery. Using the modification, Dr. Jobe performed 33 more operations, with only a 5 percent occurrence of ulnar nerve paresthesia (Thompson et al. 2001). About 12 or 15 years ago we got better drills and better tools and started not [moving the ulnar nerve out of the way] and being able to do the procedure without touching it, Jobe said. That turned the corner and we almost have no complications now. (Greenfield and Rogers 2000).
Of the 12 orthopedic surgeons I surveyed, 4 (33.3%) regularly transpose the ulnar nerve (Figure 13). However, if a player is experiencing ulnar nerve problems before surgery, the ulnar nerve may need to be transposed. Also, Dr. Cain and Dr. Dugas from the American Sports Medicine Institute in Birmingham, Alabama state that they remove the median intermuscular septum from the humerus so that it wont impinge on the nerve when it is transposed.
Bone Anchor Method
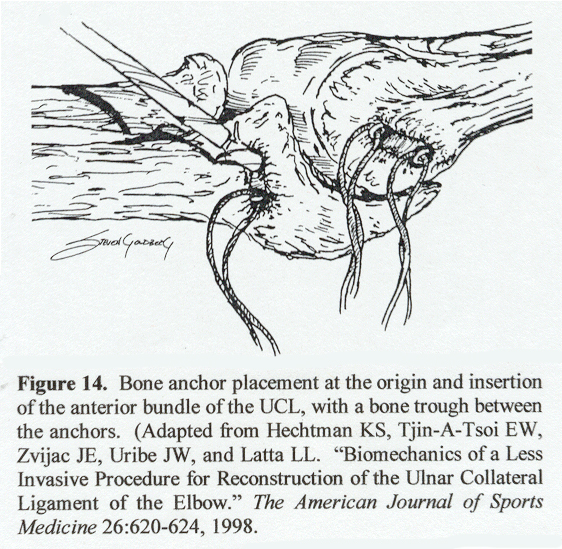
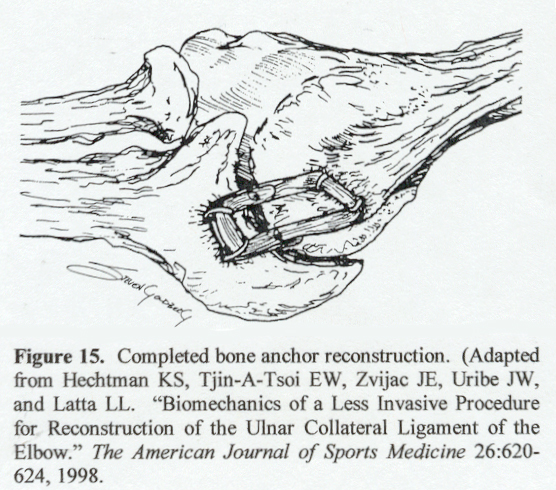
The innovative bone anchor technique was described by Hechtman et al. (1998) as an alternative to the bone tunnel technique. In the bone anchor procedure, the UCL is exposed via a muscle-split of the flexor-pronator allowing the surgeon to avoid an ulnar nerve tranposition. To create the anchors, a transverse bone trough is made on the anteroinferior surface of the medial epicondyle of the humerus, the site of the UCL anterior band origin. Then anchors are placed on the medial and lateral border of the trough. Next, a vertical bone trough is created on the sublime tubercle of the ulna, the location of healthy UCL insertion. Anchors are positioned at the anterior and posterior borders of the trough (Figure 14). Once the four anchors are in place, the tendon graft is attached to the medial epicondyle with sutures. The graft is then pulled taut and fastened to the tubercle, and then the ends are attached back to the graft, pictured in Figure 15 (Hechtman et al. 1998).
In a study assessing the UCL replacement techniques, the normal and bone anchor groups were tight while the bone tunnel group was lax toward extension. Furthermore, the anterior band strain was lax in normal and bone anchor groups and tight in the bone tunnel group toward flexion (Hechtman et al. 1998). Normal elbows in the experiment had a mean valgus load strength of 22.7 ± 9.0 Nm. The bone tunnel strength was 76.3% of that value while the bone anchor strength was 63.5% of the original elbow strength. While the bone anchor and bone tunnel group were considered significantly weaker than a healthy elbow, they were not significantly different from each other (Hechtman et al. 1998). Thus, the bone anchor group was considered a more accurate approximation of the original ulnar collateral ligament anatomy without having a significant difference in reconstructed ligament strength.
Docking Procedure
Another new method currently being used to reconstruct ulnar collateral ligaments is the docking procedure described by Hyman et al. (2001). This has altered bone tunnels and thus no longer uses figure-of-eight graft passage. The ulnar tunnels are similar and are positioned on the ulna at the anterior and posterior margins of the sublime tubercle using a 3.2-millimeter drill bit.
The bone tunnels on the medial epicondyle, however, are not the same as the divergent holes from a single entry hole that Dr. Jobe originally used. Instead, a 3.2-millimeter drill makes a single cylindrical hole in the medial epicondyle 15 millimeters long. Then, two small 2.0-mm divergent drill holes, 5 to 10 millimeters apart, are made in the proximal anterior cortex of the epicondyle and enter into the 15-mm tunnel (Hyman et al. 2001).
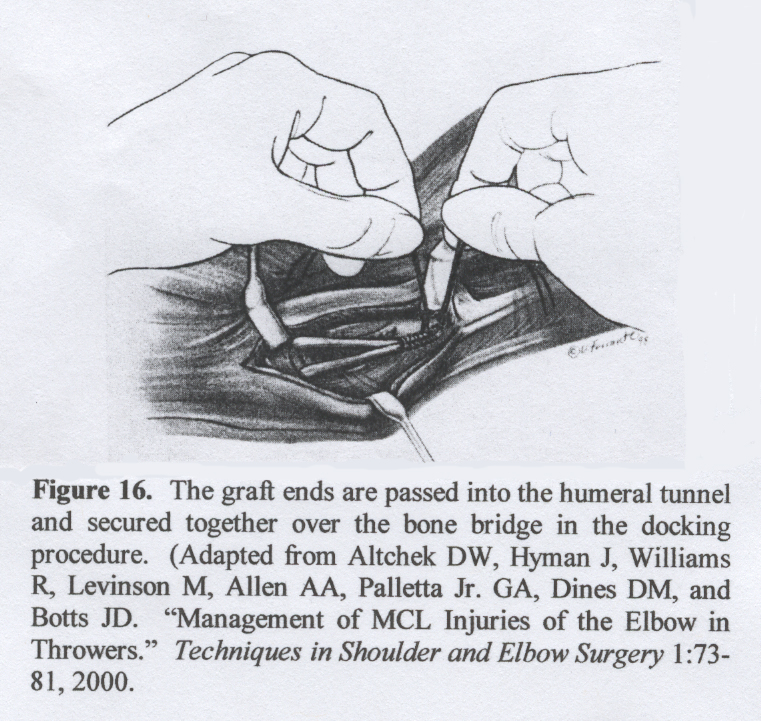
The graft is then passed from anterior to posterior through the ulnar tunnel and the tendon end with sutures is passed into the large humeral tunnel and through one of the small humeral tunnels. Subsequently, the final length of the graft is measured by estimating the length of the graft that will allow it to fit through the humeral tunnel and placing a #1 braided nonabsorbable suture at that location (Hyman et al. 2001). This end of the graft is then pulled through the humeral tunnel and in a similar fashion as the other end. If the surgeon is satisfied with the graft tension, the two sutures are tied over the bone bridge on the epicondyle (Figure 16). Hyman, Breazeale, and Altcheck (2001) believe the docking procedure is best due to the ease of graft tensioning and secure bone bridge fixation. Using this procedure, 29 of 30 (97%) baseball players have returned to the level of play they were at before surgery.
|